What are family-based placements?
Children belong with family. Child protection agencies and their community-based partners should exhaust all means necessary to support children’s safety and the family’s stability in order to prevent family separation. When temporary removal is needed to ensure the safety of the child, placing children with kin — biological relatives or chosen family (fictive kin) — is the best option. Child protection agencies must work to identify and engage family to ensure children are not separated from siblings, relatives, and communities. When this is not possible, the next best placement option is in a non-kinship, family-based setting, which provides children with access to nurturing relationships in a supportive and stable environment until they can be reunited with family.
When considering the best family-based setting, it’s important to remember that each child has unique needs and may require different approaches to out-of-home care and support. Agency leaders must ensure that current and prospective caregivers are well-informed about children’s needs, and how their specific caregiver responsibilities support the diverse needs and strengths of children. Resource families1 at all levels also must be provided with sufficient resources tailored to the child’s unique needs to support stability and healing. Clearly defining different family-based settings helps resource parents choose roles that best align with their skills and interests and ultimately improve their effectiveness and satisfaction.
This brief outlines common types of family-based settings for children in foster care, highlighting differences between resource caregivers and input from individuals with lived experience.2 Some jurisdictions offer multiple levels and types of family-based settings, while others, such as New Jersey, have implemented a single family-based system of care that includes enhanced resources and wraparound services targeted at the child and family’s unique needs. California recently moved to an innovative tiered rate structure to provide children in family-based settings the same level of funding to support their care and supervision, strength-building, and immediate needs regardless of the placement type. Ultimately, there is no single way to approach family-based placements. Each jurisdiction must work with lived experts, providers, and other community stakeholders to determine what is best to ensure a sufficient inventory of kinship and non-kinship family-placed settings for children in foster care. For more information, see: What are some strategies for finding and keeping resource families? and How have some child protection agencies recruited and retained resource families?
Diverse children need diverse families
Children placed in loving, nurturing family settings have better outcomes compared to those in group homes and institutions. They have fewer placement moves, spend less time away from family, are more likely to be placed with their siblings, remain near their community of origin, and have lower anxiety levels.3,4 In contrast, a breakthrough report on youth experiences in group and institutional placements described many non-family settings as punitive, prison-like, and traumatic. These settings often failed to offer consistent, caring relationships and even prevented young people from building relationships deemed essential for healing and a successful transition to adulthood. Research shows that Black and multiracial children often are overrepresented in group and institutional placements.
To ensure children are placed with a nurturing family instead of a facility, it is important to recruit and retain high-quality resource caregivers of all types —kinship, emergency, respite, therapeutic, treatment, specialized, medical, and professional. Using data-driven, targeted recruitment efforts increases the likelihood of identifying caregivers that mirror the varied backgrounds and social identities of children in foster care. African American and American Indian/Alaska Native children are overrepresented in foster care. Although African American children make up 14% and American Indian/Alaska Native children make up 1% of the U.S. child population, they are disproportionately represented in foster care, accounting for 23% and 2% of foster care placements, respectively. Among older youth, LGBTQ+ and pregnant and parenting teens often encounter placement instability. Having a diverse pool of resource families increases the likelihood that children and older youth are placed in a family-setting that best supports their holistic needs, cultural background, and social identity.
Many children in the child welfare system have intensive behavioral and emotional needs. Some children enter foster care with preexisting behavioral health conditions, which can be compounded by the emotional traumas associated with family separation and placement. Research shows that securing stable placements for children with complex behavioral health needs can be challenging,5 and children with clinically significant trauma are likely to experience a higher rate of placement instability.6
Children with medical complexities — defined as having functional limitations, at least one chronic condition that is severe and associated with fragility, and high healthcare needs and utilization7 — make up another growing population of children in foster care, representing about 10% of all placements. These children require tailored post-placement support to meet their needs.
Some states still lack a clear and consistent distinction between therapeutic and medical foster care settings, as children with mental or behavioral needs often are grouped with those who have severe medical and physical needs. Although therapeutic and medical foster care may offer similar services to address children’s intensive needs, research emphasizes the necessity of defining and identifying children with complex medical needs8 not only to improve the quality of support and services, but also to accurately track this vulnerable population within child welfare data systems.
It is important to keep children with family or at least in their communities when they are being placed. When I was dealing with child welfare, the child was placed far away from where she was raised. Placing kids in their community is about keeping them in their culture with people who know and understand their background.
– Samaris Rose, Resource and Adoptive Parent, Maine
Different types of family-based placements
While the concept of foster care is fairly straightforward, there are varying levels, tiers, and types of family-based placements. When a child cannot remain safely at home, child protection agencies must carefully identify the most suitable, family-oriented setting. While terms may vary, examples of the range of family-based placements offered throughout the country fall into certain categories, highlighted below:
Kinship care is the preferred family-based placement when children must be removed from their home. Placing children with kin, whether biological relatives or fictive kin (chosen family), helps minimize trauma due to separation from parents while maintaining family connections, increasing placement stability, and upholding cultural values and identity.9 Kinship placements can occur either with traditional or therapeutic/treatment resource families. When kinship placement is not an option, only then should child protection agencies consider placing children in a family setting with non-kinship resource caregivers. Those caregivers nevertheless must provide children with tangible connections with their community and extended family, and support safe family reunification when possible.
Emergency foster families are resource caregivers who provide immediate, short-term placement for children entering foster care. They typically are prepared to accept a child at moment’s notice, as some are considered to be “on call” as an emergency placement option. While children are in emergency placement, child protection agency staff must work diligently to identify a more permanent placement solution, ideally a kinship caregiver. If that is not possible, the child may be placed with a non-relative resource family.
Treatment resource families, also known as “therapeutic” or “specialized” foster parents, are resource caregivers who typically are engaged to care for children with complex emotional, behavioral, or psychological needs, in many instances resulting from trauma. Treatment caregivers receive a range of specialized education and training, including behavioral management and trauma-informed, therapy-based approaches to support children’s healing and help them develop essential coping skills. Unlike traditional resource caregivers, treatment caregivers generally care for one or two children at a time, and must work closely with caseworkers, schools, and mental and behavioral health care providers to offer intensive support. These resource parents are required to access and implement individualized treatment plans, which typically rely on a wide range of care management tools such as individual and family therapy, medication management, in-school supports, and enhanced case management. In support of a kin-first culture, there are emerging approaches that support relatives and chosen family as treatment caregivers. The Family Focused Treatment Association provides consultation, technical assistance, and resources, such as The Kinship Treatment Foster Care Initiative Toolkit, to help agencies engage, support, and train family members as therapeutic caregivers. The association also developed and piloted the Kinship Therapeutic Foster Care model in North Carolina, providing basic resource caregiver training and therapeutic caregiver licensing to relatives and chosen family.
Professional resource parent is another term used to reflect a higher level of family-based care, whereby a skilled individual provides full-time care for children with complex needs while managing intensive therapeutic supports and interventions. Professional resource parents often are from fields such as medical health, behavioral health, education, or social work, and receive specialized training that may include 30-plus hours of pre-service and 15-plus hours of annual in-service training. Professional resource parents attend all care management meetings (such as psychiatric, educational, court, and health), and work closely with child protection agency staff and other professionals to ensure comprehensive treatment and care. Professional caregivers generally provide time-limited placements for one youth at a time, for 90 days up to 26 months, and typically are not considered permanency resources.
Medical foster care is offered in various states, including Alabama, Florida, Georgia, and Washington, ensuring children with complex or chronic health conditions, physical limitations, and developmental delays receive targeted services and support. Similar to therapeutic caregivers, medical resource caregivers are extensively trained to support children with severe medical conditions such as those that contribute to neurological and functional decline, traumatic spinal cord injury, and quadriplegia. Medical resource caregivers provide around-the-clock home-based care, with assistance from parents, child protection agency caseworkers, registered nurses, clinicians, and other health professionals.
All caregivers need a break from time to time, especially families caring for large sibling groups or children with complex needs. Respite caregivers provide relief to full-time resource parents who may need a break. Respite care can occur in-home or out-of-home, and can be offered for a few hours, overnight, or weeklong. Whether it is prescheduled or in response to a crisis, respite care plays a vital role in the well-being of resource parents and the children in their care, giving both an opportunity to reset without a placement disruption.
Some distinctions and considerations
While resource caregivers play a vital role in providing safe and loving environments for children until they can safely return to their families, there are differences and considerations between each resource caregiver role. Child welfare staff must ensure that those who are interested in becoming a resource caregiver — regardless of the level or type — understand the functions, key competencies, and scope of training required to fulfill their roles, as well as the range of services available to them.
Required trainings
Each jurisdiction implements its own policies and practices regarding resource caregiver training. The scope of training can vary widely based on the number of required hours, the learning format (instructor-led, self-guided, in-person, virtual, or hybrid), and core topics. Most states, including Tennessee and Minnesota, require traditional resource families to complete comprehensive training sessions covering a variety of topics including an overview of the child welfare system, how to work with parents, behavioral management, and understanding trauma. Treatment or professional resource caregivers, however, are required in every state to undergo in-depth training that includes techniques in managing aggressive behaviors, therapeutic communication, trauma-informed care, crisis intervention, and administering medication. Ongoing training related to the needs of the specific child in care also often is required. While training programs may vary between jurisdictions, the ultimate goal is the same — to ensure therapeutic resource families can provide children with high emotional, behavioral, or mental health needs the care and support they need to thrive while in foster care. New York maintains a clear distinction between traditional, therapeutic, and emergency resource families, specifically requiring emergency caregivers to complete an additional 15 hours of specialized training and a minimum of six hours of follow-up training each year.
Some states have integrated their training requirements for caregivers, no matter their role. In Texas, all resource families — therapeutic or traditional — have mandatory training in first aid and CPR, psychotropic medication, and behavior management. This movement reflects advocates’ concerns that some traditional resource families may not possess the tools necessary to navigate the behavioral and psychological consequences of trauma through basic training alone, despite the high prevalence of significant traumatic experiences among children in foster care.
Compensation
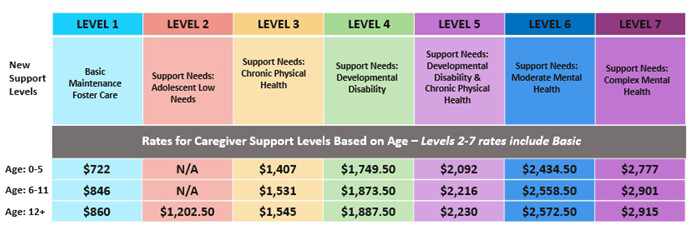
Each state has its own compensation rate structure for resource caregivers, which often is determined based on the level of care the child needs. Traditional resource families typically receive stipends that cover basic living expenses. Treatment resource parents, however, are compensated at a higher rate due to the additional training required, and some professional resource caregivers receive a stipend or salary to cover the costs of staying home to provide full-time supervision and treatment care. The new tiered rate structure in California reflects a shift away funding being based on placement type to that of a child’s needs. This reform ensures that children receive support commensurate with their individual assessed needs and strengths, as determined by the Child and Adolescent Needs and Strengths assessment. Washington has implemented a seven-level caregiver support model outlining foster care payment rates for resource caregivers. In Milwaukee and the District of Columbia, individuals may be hired as stay-at-home, full-time professional caregivers for a multi-year commitment, in lieu of other employment.
{kind=link}
California’s Foster Care Rate Structure
California’s new needs-based rate structure for its foster care system includes four tiers, each with three funding categories: 1) care and supervision; 2) strengths building and maintenance; and 3) immediate needs. This innovative structure is designed to support the child’s safety and well-being, regardless of placement setting. For example, resource caregivers of children with relatively low needs receive $1,788 per month for care and supervision, while those caring for children with the highest needs may receive up to $6,296 per month, along with additional funding for immediate needs and administrative support. This approach aims to promote family-based placements, reduce reliance on group settings, and address historical inequities in the foster care system.
Certainly, providing holistic support to meet children’s essential needs (such as clothing, food, and a stable living environment) requires a commitment that often comes with expenses. While compensation ensures caregivers have financial support to properly care for children, it’s important to consider the negative perception of the term “paid professional” for resource caregivers. An intimate bond can develop between resource families and children while living together in a family setting. The term “paid professional” may cause some children and families to believe there is a lack of commitment or authenticity to their relationship with a caregiver, because the person may be perceived as only doing a job versus genuinely supporting them. Although the idea of a salaried professional resource caregiver may be controversial to some, the fact remains that financial support is essential to providing safe, stable, and supportive placements for children, including those who need around-the-clock care and supervision to stay safe within a family-based setting.
When recruiting new families, it is important to understand their motives for becoming resource parents. There is a big misconception that resource families are supposed to adopt the child in their care, but that is not why they exist. Resource families need to know their role, which is to support children and their family until they can be reunited.
– Pasqueal Ngyuen, Parent, Louisiana
Caring for the whole family
The ultimate goal of foster care is safe family reunification. Timeframes vary for when children can be safely reunified with their biological or primary caretaker, but separation from family for any amount time can be a traumatic experience for children. Resource caregivers often are a bridge between children and their parents by supporting the whole family’s best interests and the child’s well-being, while helping to keep family connections intact until safe reunification is possible.
Placing siblings together should always be the top priority as it is vital to preserving sibling connections. Traditional resource families can care for multiple children at a time, making this family-based setting an ideal placement for a sibling group. These families, however, may need additional resources and supports to accommodate a larger sibling group, in terms of more space and transportation assistance, and this can make the placement unfeasible. Although group settings are not ideal placements, they sometimes offer the only viable option to keep a sibling group together. For instance, a few programs—such as SOS Children’s Villages in Illinois and Florida, and Boys Town — allow professional resource parents to care for sibling groups of up to six children.
Supporting parents and siblings sometimes can be achieved through a shared family care model in which parents and their children live together within a resource family, or a resource caregiver provides the parents formal mentorship. These professional caregivers commit to coaching and mentoring parents, building co-parenting relationships, and supporting a child’s transition home, including the provision of aftercare services to support permanency over time. While this approach may not be common practice among professional resource parent programs, Neighbor to Family is a promising, research-supported program that keeps sibling groups and parents together in a single home, under the care and support of a professional resource caregiver. Nexus Family Healing also provides a range of services for children — including foster care, behavioral and mental health, and residential treatment — to support families during challenging times. The program’s goal is to help families heal from trauma, and a key part of that healing is to keep families connected and engaged while children receive the treatment and care they need.
Strong parent and caregiver connections help to support positive co-parenting relationships while helping to minimize the trauma associated with family separation. Various jurisdictions implement a range of strategies to help clarify the caregiver role and build rapport and trust to strengthen the connection between caregivers and parents. Iowa employs Quality Parenting Initiative activities, such as comfort calls, to allow caregivers and parents to exchange pertinent information regarding the placement, the child’s ongoing care needs, and strategies to ease the child’s adjustment to a new placement. In North Carolina, a shared parenting policy has helped to strengthen partnerships between parents and resource caregivers and maintain connections to a child’s culture, traditions, and routines. Parents and caregivers are required to meet within 14 days of a child’s removal from the home to share information and care strategies to help lessen the stress of family separation until safe reunification is possible.
Resource parents should be aware that kids can be reunited with their families, even if they do not think the child should return home. Reunification is a part of the process. Knowing this upfront will help weed out people who have different motives for becoming a resource parent.
– Bob Ruble, Kinship Caregiver, California
1 The terms “resource caregivers” and “resource families” is used rather than “foster parents” and “foster families” to reflect their broader role and more inclusive role. In addition to providing safe and loving family-based care, they also support reunification with the child’s birth family, when appropriate. Whether relatives, fictive kin, or non-relatives, resource caregivers are instrumental in helping maintain a child’s family connections and offering support to the child’s biological family during care.
2 Content of this brief was informed through ongoing consultation with members of the Knowledge Management Lived Experience Advisory Board. This team includes youth, parents, kinship caregivers, and foster parents with lived experience of the child welfare system who serve as strategic partners with Family Voices United, a collaboration between FosterClub, Generations United, the Children’s Trust Fund Alliance, and Casey Family Programs. Members who contributed to this brief includes: Lisa Myles, Pasquel Ngyuen, Samaris Rose, Bob Ruble
3 Barth, R.P. (2002). Institutions vs. foster homes: The empirical base for the second century of debate. Chapel Hill, NC: UNC, School of Social Work, Jordan Institute for Families
4 Portwood, S. G., Boyd, S. A., Nelson, E. B., Murdock, T. B., Hamilton, J., & Miller, A. D. (2018). A comparison of outcomes for children and youth in foster and residential group care across agencies. Children and Youth Services Review, 85, 19-25.
5 Jedwab, M., Xu, Y., Keyser, D., & Shaw, T. V. (2019). Children and youth in out-of-home care: What can predict an initial change in placement? Child Abuse & Neglect, 93, 55–65.
6 Clark, S. L., Palmer, A. N., Akin, B. A., Dunkerley, S., & Brook, J. (2020). Investigating the relationship between trauma symptoms and placement instability. Child Abuse & Neglect, 108, 104660.
7 Cohen, E., Kuo, D. Z., Agrawal, R., Berry, J. G., Bhagat, S. K. M., Simon, T. D., & Srivastava, R. (2011). Children with medical complexity: An emerging population for clinical and research initiatives. Pediatrics, 127(3), 529–538.
8 Chung, J., Pecora, P. J., Sinha, A., Prichett, L., Lin, F., & Seltzer, R. R. (2024). A gap in the data: Defining, identifying, and tracking children with medical complexity in the child welfare system. Child Abuse & Neglect, 147, 106600.
9 Grandfamilies.org (2021). Kinship caregiving options: Considerations for caregivers.